Overview of Lymphoma
Lymphoma is a type of cancer that originates in the lymphatic system, a network of vessels, nodes, and organs (like the spleen and bone marrow) that helps fight infections by producing and circulating lymphocytes—white blood cells crucial for immunity. In simple terms, lymphoma occurs when these lymphocytes grow uncontrollably, forming tumors that can spread throughout the body. Unlike solid tumors, lymphoma often presents as swollen lymph nodes but can affect any organ. There are two main categories treated by lymphoma specialists in Surat like Dr. Dhruv Mehta:
-
Hodgkin Lymphoma (HL) Accounts for about 10-15% of cases. It's more common in young adults and has excellent cure rates (>80%).
-
Non-Hodgkin Lymphoma (NHL) — A broader group (85-90%), including subtypes like diffuse large B-cell lymphoma (DLBCL, most common), follicular lymphoma (indolent), and Burkitt lymphoma (aggressive). NHL varies widely in behavior, from slow-growing to rapidly progressing.
Risk factors include weakened immunity (HIV, transplants), infections (Epstein-Barr virus for HL/Burkitt), autoimmune diseases, chemicals (pesticides), and family history.
Clinical Presentation
Lymphomas often masquerade as infections like tuberculosis or allergies, delaying diagnosis by 3-6 months in India. The most common presentation is painless swelling in the neck (cervical, 60%), armpits (axillary), or groin (inguinal). Other symptoms like fever >38°C, night sweats soaking clothes, and weight loss signal advanced disease in 30-40% of cases. Some patients develop itching after alcohol consumption in HL. In advanced stages, chest pain, facial swelling, left upper abdominal pain due to splenomegaly, anemia, and bruising are common complaints. In aggressive forms of NHL like DLBCL, there is rapid growth of lymph nodes, abdominal pain, skin rash, headache, or seizures. Indolent forms of NHL, like follicular lymphoma, are mostly asymptomatic for weeks and are accompanied by easy fatigability as a symptom. Sometimes lymph nodes may wax and wane over time. Diagnosis of lymphoma should be suspected when lymph nodes persist for more than 4 weeks and are associated with fever, night sweats, weight loss, and anemia.
Diagnosis
Diagnosis of lymphoma by a lymphoma specialist in Surat like Dr. Dhruv Mehta requires tissue confirmation; imaging and lab investigations guide therapeutic decisions. CBC, LDH, beta-2 microglobulin, HIV/HBV serology, and flow cytometry are some of the lab tests done. PET-CT is the gold standard investigation done for staging of lymphoma. Removal of the whole node or excisional biopsy is required for confirmation, followed by an immunohistochemistry test for subtyping. Molecular testing may further be advised depending on the type of lymphoma for further prognostication.
Treatment With Lymphoma Specialist In Surat
Choosing the right therapy offered by a lymphoma specialist in Surat like Dr. Dhruv Mehta is crucial for improving the response rates and overall survival of the patient. Which therapies are to be chosen and in which combination is decided by oncologist Dr. Dhruv Mehta depending on the patient’s stage, comorbidities like diabetes, hypertension, heart problems, etc., and subtype of lymphoma. Lymphomas are curable in 70 to 80% of the cases.
- For HL, the ABVD protocol for 6 months or escalated BEACOPP in high-risk cases with involved site radiation in early stages. In relapsed Hodgkin lymphoma cases, targeted therapy like brentuximab vedotin (anti-CD30 monoclonal antibody) may be advised with autologous stem cell transplant.
- For aggressive NHL like DLBCL, the R-CHOP protocol is advised. Your oncologist may advise watchful waiting for indolent NHL like follicular lymphoma. Sometimes intensive chemo protocols may be advised for aggressive NHL like Burkitt lymphoma. Allogeneic bone marrow transplant is an option in relapsed NHL.
By 2025, lymphoma treatment has shifted from cytotoxic chemo to precision modalities, improving outcomes 20-40% in refractory cases. Targeted therapies like ibrutinib or acalabrutinib for mantle cell lymphoma have overall response rates up to 70%. Venetoclax, a newer targeted drug, has shown complete response rates of 80% in follicular NHL. IMMUNOTHERAPIES have shown responses of approx. 70% in relapsed/refractory HL. A game-changer therapy for relapsed or refractory NHL is CAR-T cell therapy, where a patient’s T-cells are engineered to express chimeric antigen receptors targeting specific antigens (CD19).
Follow Up Care With Lymphoma Specialist In Surat
After completion of therapy with a lymphoma specialist in Surat Dr. Dhruv Mehta, long-term follow-up is required to detect recurrences and second primary cancers and to look for late toxicities of chemotherapy and radiation. It is important to watch for symptoms that could signal the return of cancer—headaches, convulsions, shortness of breath, chronic cough, bony pains, abdominal pain or distension, jaundice, weight loss despite adequate food intake, etc. The general schedule for checkups is 3 monthly in the first 2 years, 6 monthly between years 3 and 5, and annually after 5 years. Also, lifestyle modifications like quitting tobacco/alcohol, maintaining a healthy weight (BMI <25), exercising 150 min/week, eating plenty of fruits and vegetables, and limiting red meat are advised. HPV and EBV vaccines, HIV control, and safe pesticide use are some preventive measures one can undertake.
Lymphoma, once ominous, is now largely beatable—75,000 Indians will face it in 2025, but 60% will survive 5+ years with vigilant care. From node swelling to CAR-T triumphs, knowledge bridges gaps. Advocate screening, support research—together, we outsmart cancer.
Overview of Multiple Myeloma
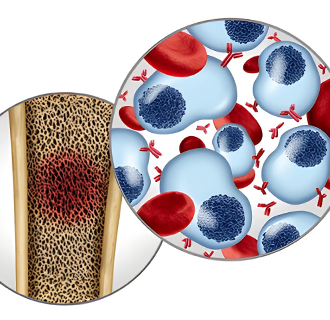
Multiple myeloma (MM) is a type of blood cancer that affects plasma cells, a kind of white blood cell produced in the bone marrow responsible for making antibodies to fight infections. In MM, these plasma cells become cancerous, multiplying uncontrollably and crowding out healthy blood cells. This leads to weakened immunity, anemia, bone damage, and kidney problems. Think of it as a factory malfunction: instead of producing useful antibodies, the rogue cells churn out faulty ones (M proteins) that harm the body.
MM is the second most common blood cancer worldwide, after non-Hodgkin lymphoma. In India almost 17,000 new cases are diagnosed, and approx. 15,000 die annually from MM. It primarily affects older adults, with a median diagnosis age of 65-70 years, though younger cases occur. Unlike some cancers with lumps, MM is "invisible" until symptoms appear, often at advanced stages. Risk factors include age, male sex, family history, obesity, radiation exposure, and conditions like monoclonal gammopathy of undetermined significance (MGUS), a precursor state in 1-2% of people over 50.
The good news? Survival has tripled in the last two decades due to better treatments offered by oncologists like Dr. Dhruv Mehta at Multiple Myeloma treatment centers —from chemotherapy to targeted drugs and immunotherapies. In India, where healthcare access varies, early detection via routine blood tests can be lifesaving. Five-year survival is 40-50% in India (vs. 60% globally), hampered by late diagnosis (70% stage II-III) and access barriers.
Clinical Presentation
MM symptoms often creep in gradually, mimicking aging or arthritis, leading to 6–12-month delays in India. About 20% are asymptomatic (smoldering MM), found incidentally. Bone pain affects 70% of patients; back/ribs/hips pain from fractures or plasmacytomas (tumors). Sudden severe pain signals cord compression, which is a true emergency. Fatigue and weakness from anemia (low red cells, 60-70% of cases) are common, resulting in pale skin and shortness of breath. Recurrent infections occur due to weak immunity; pneumonia or urinary tract infections occur due to low functional antibodies. Approximately 50% of patients develop kidney failure. Advanced signs include confusion, constipation, nausea (“stones, bones, groans, and moans”), weakness from spinal involvement, and weight loss. High-risk groups (e.g., diabetics) notice thirst or polyuria first. In India, misdiagnosis as osteoporosis or infection is common—persistent pain for more than 2 weeks should prompt a visit to Multiple Myeloma treatment centers and consult an oncologist like Dr. Dhruv Mehta.
Diagnosis
Diagnosis in Multiple Myeloma treatment centers combines labs, imaging, and biopsy; no single test suffices. Lab investigations include CBC, serum protein electrophoresis (SPEP), urine Bence-Jones proteins, calcium, creatinine, beta-2 microglobulin, and free light chain ratio (FLC). Bone marrow biopsy is diagnostic. A skeletal survey (X-rays for lytic lesions) or whole-body low-dose CT/MRI/PET-CT for high-risk may be required.
Treatment In Multiple Myeloma Treatment Centers
Treatment in Multiple Myeloma treatment center is risk-adapted, aiming for remission. Autologous stem cell transplant (ASCT) is usually advised after remission with induction chemotherapy. Long-term maintenance oral medicines are required to sustain remissions. Radiation may be given by Dr. Dhruv Mehta for painful bone lesions. 2025 marks a golden era for MM, with immunotherapies slashing relapse risks 30-50%. CAR-T cell therapy has shown response rates of 90% in relapsed MM. However, currently these newer therapies are out of reach for the common man in India. Choosing the right therapy in the Multiple Myeloma treatment center is crucial for improving the response rates and overall survival of the patient. Which therapies are to be chosen and in which combination is decided by oncologist Dr. Dhruv Mehta depending on the patient’s age, comorbidities like diabetes, hypertension, and heart problems, and his/her eligibility for bone marrow transplant.
Follow Up Care In Multiple Myeloma Treatment Centers
After completion of therapy in the Multiple Myeloma treatment centers, long-term follow-up is required to detect recurrences and second primary cancers and to look for late toxicities of chemotherapy or immunotherapies. The general schedule for checkups is monthly for the first year, every 3 months between years 2 and 5, and every 6 months thereafter. Lifelong surveillance is advised; relapse in 50-70% of patients occurs at 2-3 years. Exercise, calcium/vitamin D supplements, and infection prophylaxis are also recommended in follow-up settings.